In 12% to 21% of idiopathic scoliosis cases, the diagnosis is made between 4 and 10 years of age. Between the ages of 4 and 6 years, the female-to-male ratio of juvenile idiopathic scoliosis is 1:1. However, the ratio of female to male cases rises to between 2:1 and 4:1 in children between the ages of 4 and 10 years, and to 8:1 in children who are 10 years of age or older.1 Both right and left curves are found with equal frequency for patients younger than 6 years, but rise to a 3:1 ratio of right versus left thoracic curves after the age of 6.2
Observation is the main treatment for patients with a small curve of less than 20° to 25°. Follow-up visits are recommended every 4, 6, 9, or 12 months, depending on the patient’s age, the degree of the curve, and the characteristics of the clinical deformity.1
Curves between 25° and 50° are usually treated with bracing in this age group. Bracing can be done either on a part-time or full-time basis, depending on the size of the curve as well as the age of the child. A study completed in 1982 evaluating the success of bracing reported an excellent prognosis when part-time bracing was utilized for patients with a curve of ≤35° and rib-vertebra angle difference (RVAD)3 of ≤20°; however, curves ≥45° and RVAD of ≥20° had a less favorable prognosis for successful treatment with bracing.1
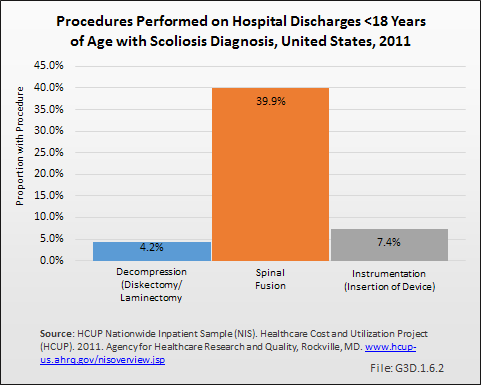
Overall, the curve patterns in patients with juvenile idiopathic scoliosis are similar to those with adolescent idiopathic scoliosis. Approximately 70% of patients with juvenile idiopathic scoliosis exhibit curve progression and require some form of treatment. In a study conducted in 1981, 55 of 98 patients (56%) with juvenile idiopathic scoliosis required spinal surgery. The most common and traditional surgery is posterior instrumentation and fusion.1
- 1. a. b. c. d. Lenke LG, Dobbs MB: Management of juvenile idiopathic scoliosis. J Bone Joint Surg Am 2007;89:55-63.
- 2. Warner WC Jr.: Juvenile idiopathic scoliosis, in Weinstein S, ed: The Pediatric Spine: Principles and Practice, ed 2. Philadelphia, PA: Lippincott Williams & Wilkins, 2001, p 330.
- 3. Rib vertical angle difference (RVAD): The rib vertical angle (RVA) is the angle formed by perpendicular line from apical vertebral end plate and a second line from the mid-neck to mid-head of the adjacent rib. The RVAD is the difference between the two RVA on the concave and convex sides of the curve. A curve greater than 20 is considered progressive. Available at: http://www.wheelessonline.com/ortho/congenital_scoliosis_and_vertebral_defects. Accessed October 22, 2014.
Edition:
- 2014
 Download as CSV
Download as CSV