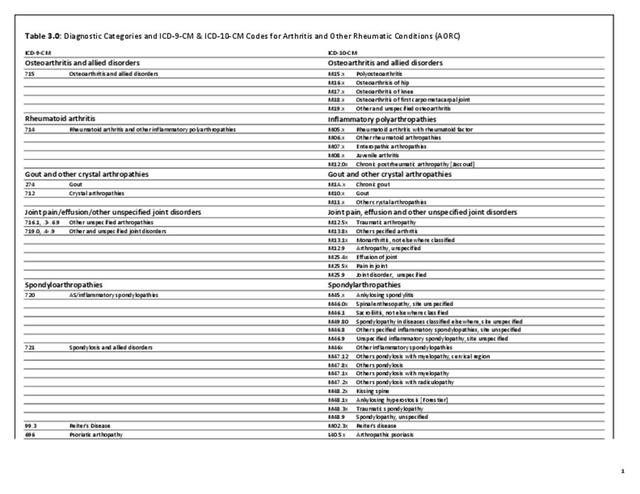
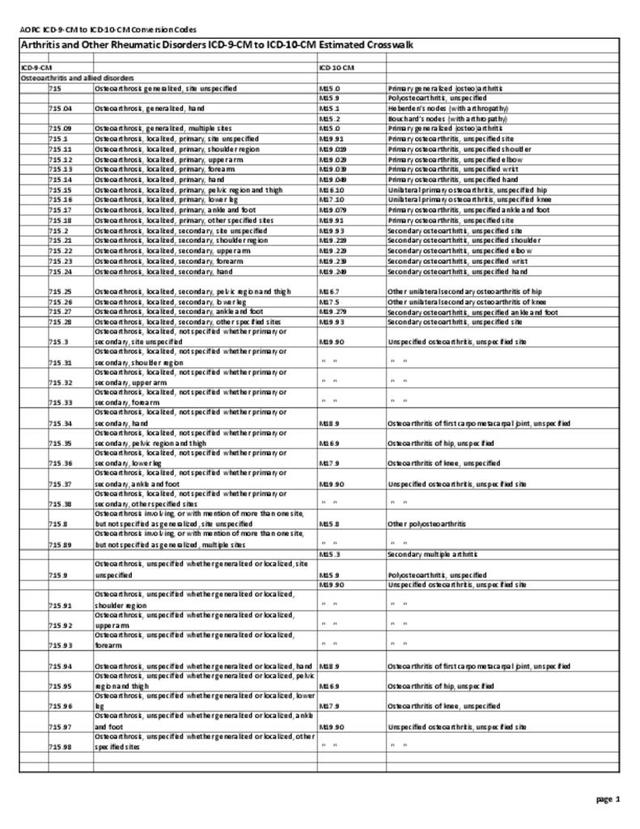
Several data limitations exist for monitoring AORC burden in the future. First, on October 1, 2015, ICD-10-CM was required for use in clinical records; it was previously in use for death records. The current National Arthritis Data Workgroup definition of AORC uses ICD-9-CM codes. Due to significant changes in conceptualizing the new codes, a direct translation cannot be made. This means a new definition of AORC or some similar concept will be needed for analyses using ICD-based data in the future. CDC is working with ICD-10-CM translation experts and selected stakeholders to propose a draft standard ICD-10-CM based definition, which will be shared with the larger arthritis community to reach agreement on a new definition.
Second, there is a need for data on more specific conditions, for example rheumatoid arthritis, systemic lupus erythematosus, and psoriatic arthritis, to help drive clinical (eg, treatment, quality of care) and public health (eg, self-management education, safe physical activity) efforts that allow for better incidence estimates in order to better understand risk. Electronic health records may prove helpful in creating valid measures. There is also a lack of data on patient reported outcome measures (PROMs) on pain and function in electronic health records and administrative databases. These outcome measures are important to assessing the impact/burden of rheumatic and musculoskeletal diseases.
Arthritis and other rheumatic conditions are not addressed with the same priority as many other chronic conditions, perhaps because such priorities are driven more by easily available measures of mortality rather than by more challenging measures such as quality of life, disability, and impact on work. However, there is a growing policy interest in the role of multiple chronic conditions in health and health costs,1 and AORC plays a major role from this perspective for at least three reasons. First, those with priority chronic conditions are highly affected by AORC, with about half of adults with heart disease or diabetes and about a third of adults with obesity affected by DDA.2,3,4 Second, arthritis is very common condition among individuals with two or more chronic conditions, regardless of the conditions considered.5 Third, those with arthritis as one of their multiple chronic conditions fare much worse on important life domains such as social participation restriction, serious psychological distress, and work limitations.6
- 1. U.S. Department of Health and Human Services. HHS initiative on multiple chronic conditions. http://www.hhs.gov/ash/initiatives/mcc/. Accessed October 24, 2018.
- 2. Bolen J, Murphy L, Greenlund K, et. al. Arthritis as a potential barrier to physical activity among adults with heart disease — United States, 2005 and 2007. MMWR 2009;58(7):165-169.
- 3. Bolen J, Hootman J, Helmick CG, et. al. Arthritis as a potential barrier to physical activity among adults with diabetes — United States, 2005 and 2007. MMWR 2008;57(18):486-489.
- 4. Barbour KE, Hootman JM, Murphy LB, Helmick CG. Arthritis as a potential barrier to physical activity among obese adults–United States, 2007 and 2009. MMWR 2011;60(19):614–618.
- 5. Ward BW, Schiller JS. Prevalence of multiple chronic conditions among US adults: estimates from the National Health Interview Survey, 2010. Prev Chronic Dis 2013;10:120203. DOI: http://dx.doi.org/10.5888/pcd10.120203.
- 6. Qin J, Theis KA, Barbour KE, et.al. Impact of arthritis and multiple chronic conditions on selected life domains — United States, 2013. MMWR 2015;64(21):578-582.
Edition:
- Fourth Edition